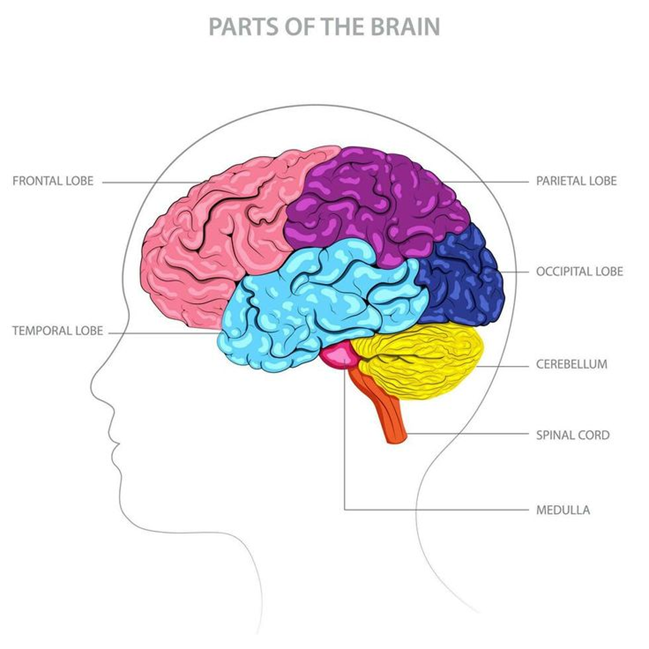
Primitive reflexes are involuntary, automatic movements that appear in a newborn from birth. These reflexes are controlled by the brainstem; a part known as the highest and most primitive part of the brain, playing a vital role in the child’s survival and development.
These reflexes shape primary movement patterns and provide the foundation for future voluntary motor skills such as crawling, walking, and writing, and of course, they play an important role in emotional regulation and learning in future cognitive development.
These reflexes are present at birth and should gradually integrate and disappear during the first year of life. As the brain matures and higher centers, especially the cerebral cortex, become active, control of movements transfers from the brainstem to more advanced parts.
Several Examples of Primitive Reflexes
1. Moro Reflex
Time of Onset: Birth
Signs: Sudden opening of arms and legs upon feeling of falling or hearing a loud noise, followed by pulling them in; often accompanied by crying.
Purpose: Protection and maintaining infant alertness.
Time of Disappearance: 4 to 6 months
Persistence: Can cause hypersensitivity to sound, light, or movement, and problems with balance and emotional regulation.
2. Rooting Reflex

Time of Onset: Moment of birth
Signs: Movement of head and opening of infant’s mouth when cheek or chin is touched.
Purpose: To find the nipple for feeding.
Time of Disappearance: Around 4 months
Persistence: May affect speech development and oral sensitivity.
3. Sucking Reflex

The sucking reflex is one of the infant’s first and most vital skills, essential for their survival and feeding. This reflex evolves during the first months of life and becomes a voluntary skill.
Time of Onset: Before birth (around 32 weeks of gestation)
Early Signs (Reflexive Sucking): As soon as any object (such as a pacifier, finger, or mother’s breast) touches the infant’s palate or lips, they spontaneously and automatically begin sucking.
Initial Purpose: Nutrition and creating coordination between breathing and swallowing.
Time of Disappearance (of Reflexive Sucking): Around 4 months. At this age, reflexive sucking gives way to voluntary sucking.
Persistence of the Reflex: If this reflex persists beyond 4 months, it can be a sign of developmental delay and lead to future problems with chewing, swallowing, and speech.
Key Difference: Reflexive Sucking vs. Voluntary Sucking (After 4 Months)
The infant initially sucks only reflexively, but as they grow, they learn to control this skill consciously and purposefully. The main difference between these two types of sucking is as follows:
Reflexive Sucking (Until around 4 months): This type of sucking is a completely automatic reaction.
How it starts: As soon as anything touches the infant’s lips, they immediately and involuntarily start sucking.
Conditions: This reflex is activated even if the infant:
Is not hungry.
Is sleepy or calm.
Voluntary Sucking (After 4 months): This is an acquired and purposeful skill that indicates the infant’s neural and muscular development.
How it starts: The child decides to suck on their own.
Related Behaviors:
Actively searches for a feeding source (mother’s breast, bottle, or pacifier).
Turns their head towards the source.
Brings it to their mouth themselves and initiates sucking.
Important Note: This transition from reflexive sucking to voluntary sucking is a major developmental milestone indicating that the child is gaining more control over their body and environment.
4. Palmar Grasp Reflex
Time of Onset: Birth

Signs: Firmly grasping a finger or object when the palm is touched.
Purpose: Preparation for voluntary grasping and hand-eye coordination.
Time of Disappearance: 5 to 6 months
Persistence: May affect fine motor skills such as writing.
5. Plantar Grasp Reflex

Time of Onset: Birth
Signs: Curling of toes when the sole of the foot is touched.
Purpose: Preparation for standing and walking.
Time of Disappearance: 9 to 12 months
Persistence: Can affect posture and walking pattern.
6. Asymmetrical Tonic Neck Reflex (ATNR)
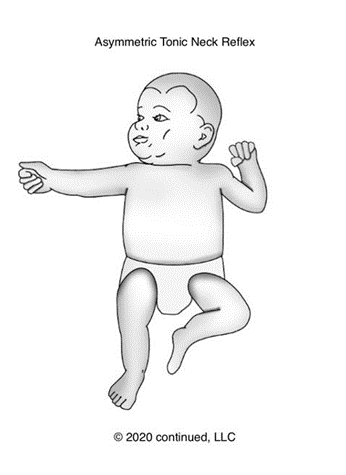
Time of Onset: Birth
Signs: Extension of the arm and leg on the side the head is turned towards, and flexion of the limbs on the opposite side (fencing posture).
Purpose: Development of hand-eye coordination, preparation for rolling.
Time of Disappearance: Up to 6 months
Persistence: May affect writing, reading, and crossing the body’s midline.
7. Tonic Labyrinthine Reflex (TLR)
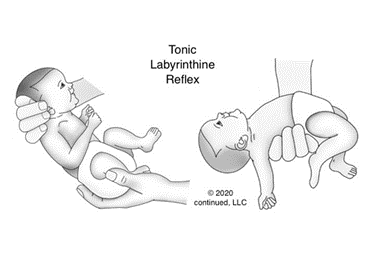
Time of Onset: Birth
Signs: Flexion of the body when the head is bent forward and extension of the body when the head is tilted back.
Purpose: Development of muscle tone, balance, and coordination.
Time of Disappearance: Up to 6 months
Persistence: Can lead to poor posture and problems with spatial awareness.
8. Spinal Galant Reflex

Time of Onset: Birth
Signs: Curving of the body to the opposite side when the spine is stroked.
Purpose: Aids movement through the birth canal and later, crawling.
Time of Disappearance: 6 to 9 months
Persistence: May be associated with bedwetting, restlessness, or sitting problems.
9. Babinski Reflex
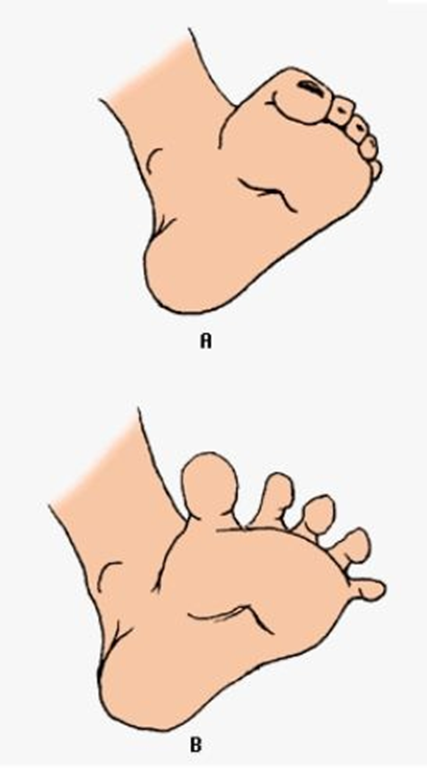
Time of Onset: Birth
Signs: Fanning of toes and upward movement of the big toe when the sole of the foot is stroked.
Purpose: A neurological indicator for examining the corticospinal tract.
Time of Disappearance: 12 to 24 months
Persistence: Can be a sign of neurological disorders.
The Importance of Primitive Reflexes
1. Survival: Reflexes such as sucking and rooting enable proper feeding and breathing.
2. Brain Development: Each reflex activates specific neural pathways and facilitates the development of the nervous system.
3. Preparation for Voluntary Movements: Foundation for crawling, walking, writing, and balance.
4. Sensory Integration: Helps in proper processing of sensory stimuli such as touch, sound, and movement.
5. Cognitive and Emotional Development: Timely integration of reflexes leads to better focus, effective learning, and emotional regulation.
6. Diagnosis of Neurological Problems: Absence or persistence of reflexes can be a sign of developmental delay, cerebral palsy, or brain injuries.
Consequences of Retained Reflexes
If primitive reflexes are not integrated at the appropriate time, problems such as:
Balance and coordination disorders
Difficulty with reading and writing
Delays in language and speech development
Weak emotional control and attention
may occur. In such cases, occupational therapy and reflex integration exercises can help the brain complete missed developmental stages.
Summary
Primitive reflexes are the foundation of a child’s motor and brain development. These reflexes appear automatically at birth, guide the first months of life, and then gradually disappear. Their timely integration is essential for lifelong motor, emotional, and cognitive health.
| Reflex name | Time of Appearance | Description | Purpose | Time of Disappearance | If it Persists |
| Moro reflex | At birth | Sudden opening of arms and legs outwards upon sensation of falling or a loud noise, followed by a return to the initial position and possible crying. | To protect the infant and maintain alertness. | 4 to 6 months | Hypersensitivity to sound/light/movement, balance issues, and emotional regulation problems. |
| Rooting Reflex | At birth | Turning the head and opening the mouth towards the point where the chin is touched. | To help find the nipple for feeding. | Around 4 months | Disruption in speech development, oral hypersensitivity. |
| Sucking Reflex | Before birth (32 weeks gestation) | Automatic sucking when an object is placed on the roof of the mouth. | To enable feeding and coordinate breathing and swallowing. | Around 4 months | Problems with chewing, swallowing, speaking, and unclear articulation. |
| Graps reflex palmar/ rabkin reflex | At birth | Tight gripping of fingers when the palm is touched. | To prepare for voluntary movements and hand-eye coordination. | 5 to 6 months | Impairment of fine motor skills (e.g., writing, picking up objects). |
| Plantar Grasp Reflex | At birth | Curling of toes when the sole of the foot is touched. | To prepare the feet for standing and walking. | Up to 12 months | Negative impact on posture and gait (walking). |
| Asymmentrical tonic neck reflex ATNR | At birth | When the head turns to one side, the arm and leg on that side extend, while the opposite arm and leg flex (resembling a fencer’s pose). | To develop eye-hand coordination and prepare for rolling over. | Up to 6 months | Difficulty with writing, reading, and crossing the body’s midline. |
| Tonic labyrinthine reflex TLR | At birth | Bending the body forward when the head is lowered down, and straightening when the head is tilted back. | To develop muscle tone, balance, and coordination. | Up to 6 months | Poor posture, clumsiness, and decreased spatial awareness. |
| Spinal gallant reflex | At birth | Bending of the body to the side when the length of the spine is stroked. | To aid in moving through the birth canal and prepare for crawling. | 6 to 9 months | Bedwetting, problems with sitting still, and fidgeting. |
| Babinski Reflex | At birth | Spreading of the toes and upward extension of the big toe when the sole of the foot is gently pressed. | A neurological test to check the development of the corticospinal tract. | 12 to 24 months | Neurological disorders in older children. |
Key Points:
Importance of Reflexes:
Survival (feeding and breathing)
Brain development and stimulation of neural pathways
Preparation for voluntary movements (walking, writing)
Sensory integration and stimulus processing
Cognitive and emotional development
Early diagnosis of neurological problems
The Importance of Primitive Reflex Integration
If primitive reflexes are not integrated and remain active beyond the expected age, they can cause impairments in:
Balance and coordination
Reading and writing skills
Speech and language development
Emotional control and attention
In such conditions, reflex integration therapies or occupational therapy can be helpful. These treatments include specific exercises designed to rebuild missed developmental stages.
Summary
Primitive reflexes are the basis and foundation of motor skills and brain development. They appear naturally at birth and disappear with brain maturation during the first months of life. The developmental stages and timing of integrating these reflexes are crucial for lifelong motor, emotional, and cognitive health.
Evidence-Based Clinical and Care Guide
What should be done, why, and how? A caregiver and child-friendly guide can provide the best environment for the natural development and integration of primitive reflexes.
Quick Summary
Creating a protective environment rich in movement
Skin-to-skin contact and a responsive environment
Reducing unnecessary stress, especially in the NICU
Encouraging varied positions and tummy time
Utilizing Kangaroo Care and developmental care protocols
Early observation and referral if reflexes persist or are asymmetrical
What Happens?
Primitive reflexes like rooting, sucking, Moro, grasp, and tonic neck are a natural part of the infant’s survival and early movement program. These reflexes usually appear during the fetal period and gradually integrate and disappear as the cerebral cortex matures.
Persistence or asymmetry of reflexes beyond the natural age can be a sign of delayed neural maturation and motor or learning problems. Early supportive care promotes normal development and neural maturation.
What Should We Do Now to Integrate Reflexes?
1. Skin-to-Skin (Kangaroo) Care
How? Frequently place the infant on the parent’s chest in a prone position from the very beginning.
Why? This promotes physiological stability, reduces stress, supports neural development, and strengthens the neuro-behavioral environment, facilitating the natural integration of reflexes.


2. Appropriate Home Routines
How? Clustered care to preserve sleep, reduce light and noise, gentle handling, caregiver attunement to the child’s needs, and using flexed (fetal-like) positions.
Why? Long-term studies show these measures promote motor outcomes and reduce stress responses, especially for infants being born (these measures should also be implemented for preterm infants).


3. Calmness and Proper Positioning at Home
How? Carrying the child in a flexed, midline position during feeding and holding; avoiding prolonged supine sleeping (e.g., in car seats); using biological nurturing and comfortable breastfeeding positions; keeping the infant’s head aligned with the spine.
Why? A flexed midline position reduces stress on the infant’s system and aids the natural transition from reflex to postural reaction. Excessive pressure or improper positioning can harm future motor development.

4. Supervised Tummy Time
How? Short, frequent sessions during the infant’s awake time; gradually increasing duration and difficulty based on tolerance; providing suitable setups for prone positioning; and two-sided play to reinforce symmetrical movement patterns.
Why? Prone positioning stimulates anti-gravity postural responses and helps the transition from primitive reflexes to voluntary movements. Evidence shows that early active movements play an important role in promoting motor developmental milestones.


At the Mother’s Health Center, our parent-child classes are founded on a fundamental principle: the integration and coordination of primitive reflexes. These reflexes, which are the cornerstone of a child’s motor and neural development, require proper integration into the nervous system for healthy and sustainable growth.
This goal is achieved through purposeful sensory and movement play. These activities help the child transform neonatal reflex patterns into more voluntary and complex movements.
Furthermore, at the Mother’s Health Center Firouzeh Roosta, for older children, if assessments reveal signs of non-integration or retention of primitive reflexes, specialized educational and interventional programs are designed and implemented to integrate these reflexes, ensuring the child’s developmental path continues in a harmonious and healthy manner.
Keywords: Pregnancy, Primitive Reflexes, Motor Development, Infant Exercise
Compiled by: Firouzeh Roosta1, Zahra Afazeli2
1: National Pregnancy Instructor, PhD in Health
f.roosta1963@yahoo.com
2: Ranked 9th in the PhD Entrance Exam in Motor Behavior, Physical Literacy Researcher
Zahra.afazeli76@gmail.com